Full time or part time? Working time preferences among registered nurses
Most of those who work part time choose to do so for reasons of lifestyle or family values. However, sociable working hours and professional challenges may provide the motivation required for some to increase their full-time equivalent percentage.
Background: The shortage of registered nurses suggests that there is a need for part time nurses to work full time. Also, earlier research shows that part-time working practices impact negatively on the quality of the service provided by registered nurses.
Objective: To shed light on the factors that influence the full-time equivalent percentages worked by registered nurses, and to gain an insight into what factors may motivate part time staff to increase their full-time equivalent percentage.
Method: Cross-sectional survey with an explorative design. Questionnaire survey among a sample of registered nurses employed by municipal and privately run institutions in a large urban municipality in Norway.
Results: A total of 206 registered nurses responded to the survey (45 per cent). Leisure time, parenting and a healthy financial situation were the most important reasons for choosing to work part time, and unsociable working hours was the most important barrier to a higher full-time equivalent percentage among part-time staff. Adjustments made by the employer would influence one group of part-time nurses, whereas another group was less inclined to be influenced by such measures. The ‘family considerations’ factor was inversely related to full-time work in that respondents were more inclined to reject full-time jobs. Sociable working hours and professional challenges provide motivation for part-time workers to increase their full-time equivalent percentage.
Conclusion: Job content, family considerations and contextual circumstances influence the full-time equivalents worked by registered nurses. For those who work part time, professional challenges and sociable working hours are factors that may motivate a change to a higher full-time equivalent percentage.
In the light of media attention on the labour force reserve of registered nurses (RNs) (1), this study sheds light on factors that influence their full-time equivalents (FTEs), and factors that may motivate part-time employees to opt for a higher FTE percentage. Part-time working practices among RNs have an adverse effect on the quality of services and the continuity of care. The professional environment suffers, and patients need to relate to a greater number of nursing staff (2–5).
In addition, part-time work means lower pay and pension earnings, and there is an adverse effect on gender equality (2, 6, 7). It is a Government objective to reduce involuntary part- time working and to promote a full-time working culture (8). It is however difficult to reduce voluntary part-time working (7) when some employees enjoy robust family finances. The wish to work part time is influenced by pressures of work and unsociable working hours, i.e. evenings, nights, weekends and public holidays (9, 10).
Earlier research
Research has shown that the reasons why RNs opt for part-time work include care roles, workload, insufficient access to full-time jobs, employer’s part-time work incentives, personal ill health and a wish to have more leisure time (7, 11). RNs will increase their FTE percentage if the employer facilitates the change and takes a flexible approach (12). Adjusting workload to work capacity, higher pay and professional challenges can be motivating factors (12, 13).
However, part-time work can sometimes be as tiring as full-time work. An unsociable shift pattern is one of the reasons (14). There is also a connection between shift work and family/work conflicts, because shift work often involves unsociable working hours which are difficult to combine with family life (14).
Efforts to increase the number of full-time positions focus on tackling the organisational culture and on introducing new ways of managing working hours and extra shifts (2, 7, 15). Research shows that RNs feel less stressed if they work longer shifts, because this brings increased continuity, a better overview, longer periods of time off work, periods of calm while at work, lower levels of stress and better patient care (16, 17).
However, international studies involving RNs who work in the primary and specialist health services show that working long shifts can impact negatively on their performance and satisfaction. There is a need for more research to be undertaken on the effect that long nursing shifts may have on patients (18–20).
The objective of the study
We need to know more about the circumstances that influence the FTEs worked by RNs, so that institutions and authorities may seek to bring about these circumstances in order to stimulate full-time working. The objective of the study is therefore to shed light on factors that influence the FTEs worked by RNs, and to gain an insight into what factors may motivate part-time nurses to accept a higher FTE percentage.
The study is based on new institutional theory, which discusses how preferences are contextually conditioned (21). Contextual circumstances such as working conditions, pay, job content and the availability of full-time positions trigger different behaviours with respect to the profession as such, and with respect to working hours in particular. The key objective is to detect and analyse influences that are generated by the nurses’ values and norms.
Method
Design
The body of data is based on a cross-sectional survey with an explorative design (22). This method was chosen because we felt an explorative approach would allow us to gain further insight into the factors that influence the FTEs worked by RNs, and the factors that motivate part-time employees to accept a higher FTE percentage. The survey was conducted in December 2013.
Sample
Survey invitations were sent to nursing homes, nursing and social care departments, psychiatric wards and medical institutions in a large urban municipality. Both private and public institutions were included. Nineteen places of work accepted the invitation to take part after they were approached in person or by phone, and all of these institutions are represented. The questionnaire was distributed to 459 RNs.
Data collection
We used a 24-point questionnaire that featured statements related to RNs’ working conditions, their professional norms in relation to choice of working time, and motivating factors. Content validity as well as face validity were considered when the questionnaire was developed (22). The questions were based on our personal knowledge of the professional field and labour research.
Eleven questions were answered by all nurses whether they worked full time or part time. The remaining 13 questions were answered only by part-time employees. Tables 1a and 2 show the questions answered by all nurses, while tables 1b and 3 show the questions answered by part-time employees only.
Statistical analyses
All questions had identical response options, ranging from ‘strongly disagree’ (value 1) to ‘strongly agree’ (value 7). The data were entered in NSDstat Pro, version 1.3 and electronically transferred to IBM SPSS, version 23. We conducted descriptive analyses, a chi-squared test, exploratory factor analysis, a t-test, binary logistic regression and odds ratio (OR) analyses (23, 24).
An odds ratio (OR) is the relationship between two odds. If OR is greater than 1, there is a positive relation, while an OR below 1 indicates an inverse relation (23). We used promax rotation because there was a correlation between the factors, and we estimated scores using Bartlett’s method (25).
Questions that loaded <0.25 were excluded from table 1. Questions that loaded on two factors were included for the factor with the highest loading. The Kaiser-Meyer-Olkin test (the KMO test) measures and compares correlation coefficients and should be greater than 0.70 (25).
Cronbach’s alpha measures the internal consistency of each factor and along the full scale (25). Values greater than 0.70 are considered acceptable (26). Missing values were recorded as the mean value of available data. The significance level was set at p ≤ 0.05.
Research ethics considerations
The questionnaire was submitted for approval to the Data Protection Official at the Norwegian Centre for Research Data (NSD), project number 35834. Notification was not deemed to be required. The local authority’s department for health and social care services approved the survey. The questionnaire and the information document were distributed to management. We had no direct contact with the informants.
The information document provided details about the survey’s objective, anonymity, voluntary participation and confidential data processing (27, 28). The return of a completed questionnaire was considered to constitute the respondent’s consent to taking part in the survey. We recorded no information that might identify an institution or an individual.
Results
Background variables
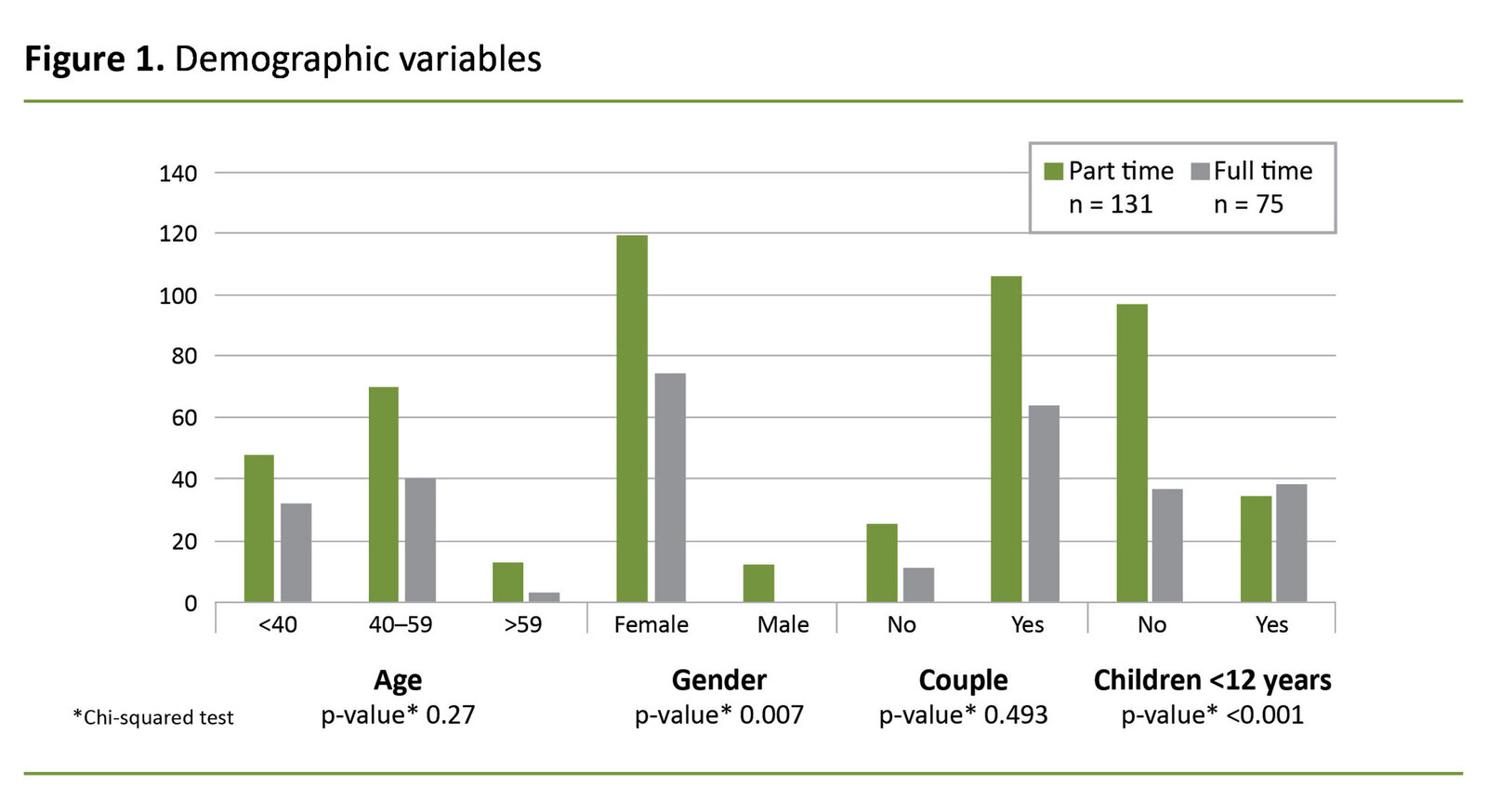
A total of 206 completed questionnaires were returned (45 per cent) distributed as follows: nursing homes 142, nursing and social care departments 41, psychiatric wards 15 and medical institutions 8. We conducted a chi-squared test to ascertain whether there were significant differences between full-time employees and part-time employees with respect to various background variables (figure 1).
The majority of respondents were living with a partner or spouse. There were significant differences between the groups in terms of parenting responsibility for children under the age of 12, and with respect to gender. The majority of respondents who were working full time did not have young children, and no men were working part time. There were few respondents above the age of 59
Factor analyses
We performed two factor analyses: one total analysis and one part-time analysis. The total analysis focused on the questions that all the nurses were asked. The part-time analysis focused on the questions that only part-timers were asked. We started out with six factors in both analyses. We found that the optimal number of factors for the explanation variance was three in the total analysis and two in the part-time analysis. No pairwise correlations between the questions were greater than 0.80.
All questions had a moderately high correlation with at least one other question, greater than 0.20. The Kaiser-Meyer-Olkin measurement (the KMO test) was 0.58 in the total analysis, which was lower than we had hoped, but it was 0.74 in the part-time analysis. Bartlett’s test showed that there were correlations between questions and that the correlations were significant in both analyses.
The combined explanation variance for three factors was 41 per cent in the total analysis, and 55 per cent for two factors in the part-time analysis. All questions loaded moderately high with at least one question per factor greater than 0.50 in the total analysis, and at least one question greater than 0.80 in the part-time analysis.
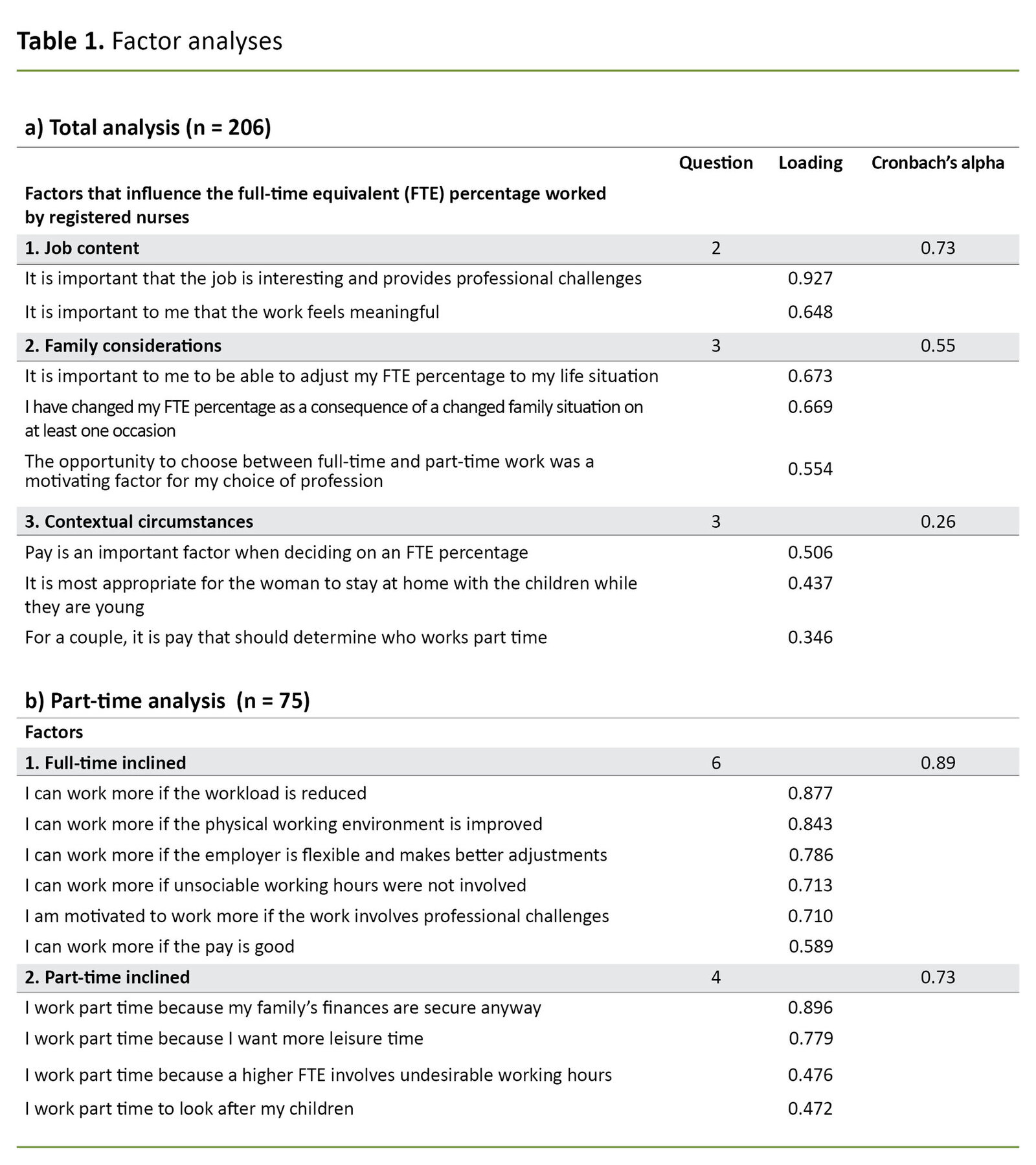
In the total analysis, Cronbach’s alpha showed a score of 0.73 for factor 1, 0.55 for factor 2, 0.26 for factor 3 and 0.38 for the full scale. In the part-time analysis, Cronbach’s alpha showed a score of 0.89 for factor 1, 0.73 for factor 2 and 0.84 for the full scale.
Factor analysis of questions answered by the complete sample
The results of the total factor analysis are shown in table 1a. The variables termed ‘professional challenges’ and ‘meaningful job’ both had a high score. These questions load on the same factor, they are interrelated and refer to job content.
Scores were also high for these statements: ‘it is important to me to be able to adjust my FTE percentage to my life situation’, ‘I have changed my FTE percentage as a consequence of a changed family situation on at least one occasion’, and ‘the opportunity to choose between full-time and part-time work was a motivating factor for my choice of profession’.
These questions concern family considerations; they load on the same factor and are interrelated. It is interesting to note that also loading on the same factor are these statements: ‘pay is an important factor when deciding on an FTE percentage’, ‘ it is most appropriate for the woman to stay at home with the children while they are young,’ and ‘for a couple, it is pay that should determine who works part time’.
These questions concern contextual circumstances. The total analysis showed that job content and family considerations had a higher loading than contextual circumstances.
Factor analysis of questions answered by part-time employees
Table 1b shows the results of the factor analysis for questions answered by part-time employees. These questions load on two factors and are interrelated. There were high scores for the variables ‘workload’, ‘physical working environment’, ‘employer’s flexibility’, ‘unsociable working hours’, ‘professional challenges’, and ‘well paid’.
The questions are suitable for operationalising circumstances that are considered to be important for the group of RNs who are full-time inclined, i.e. those who may be influenced to accept a full-time position if the employer makes appropriate adjustments. There were also high scores for the variables ‘secure finances’ and ‘wanting leisure time’.
The scores were moderately high for the variables ‘undesirable working hours’ and ‘responsibility for children’. The questions operationalise circumstances that are considered to be important for the group of RNs who are less inclined to be influenced by adjustments made by the employer, and who are part-time inclined
Reasons for the choice of full-time equivalent percentage
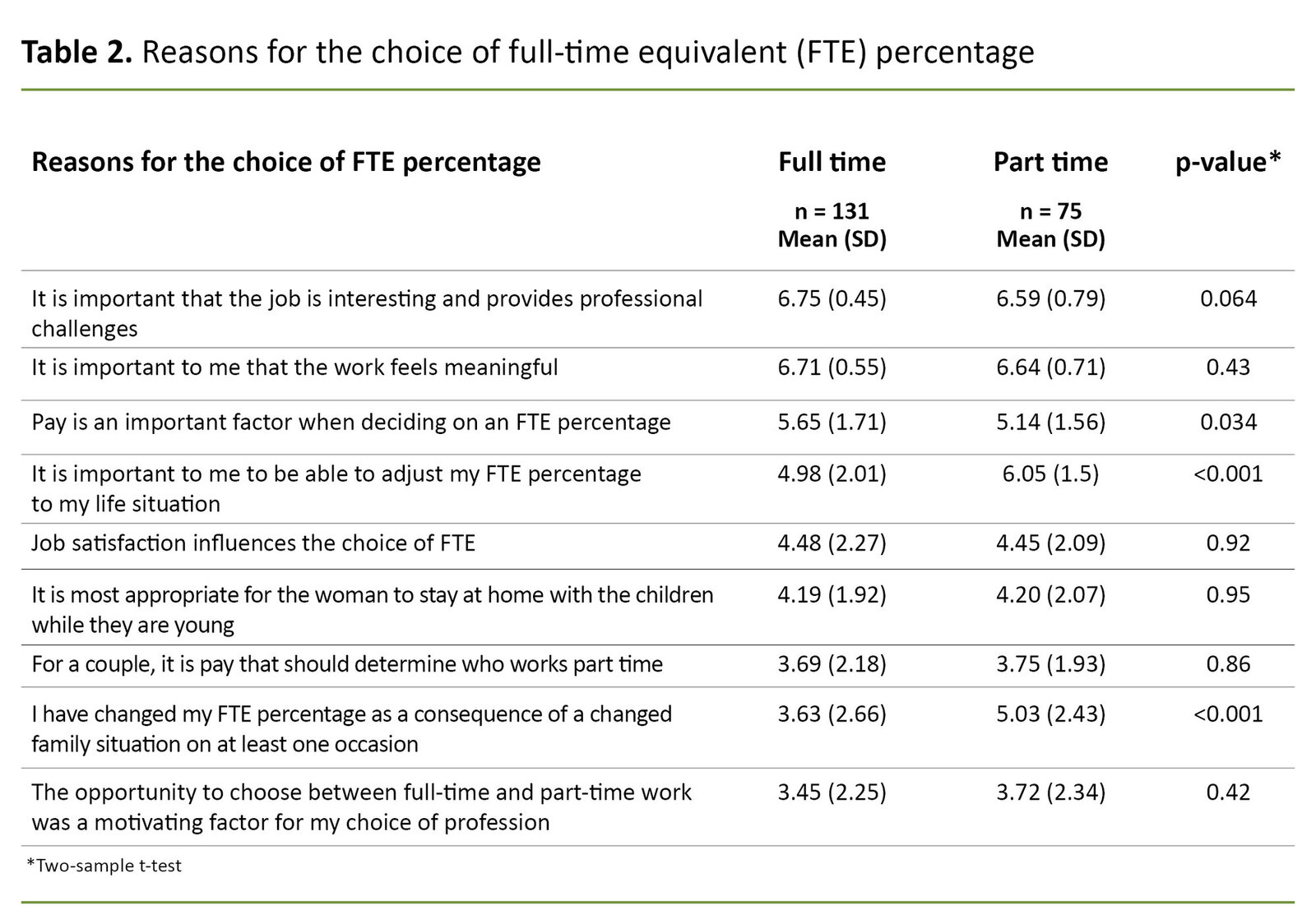
The survey questions took the form of statements about reasons for the respondent’s choice of FTE percentage. The results are shown in table 2. Professional norms appear to have the greatest impact on the choice of FTE percentage, and professionally founded reasons were prevalent in both groups.
It was less important for full-time staff than for part-time staff to be able to adjust their FTE percentage to their life situation. The mean score was lower for those who worked full time than for those who worked part time in relation to the question about having changed their FTE percentage as a consequence of a changed family situation.
Reasons for choosing to work part time and factors that motivate a decision to increase the full-time equivalent percentage
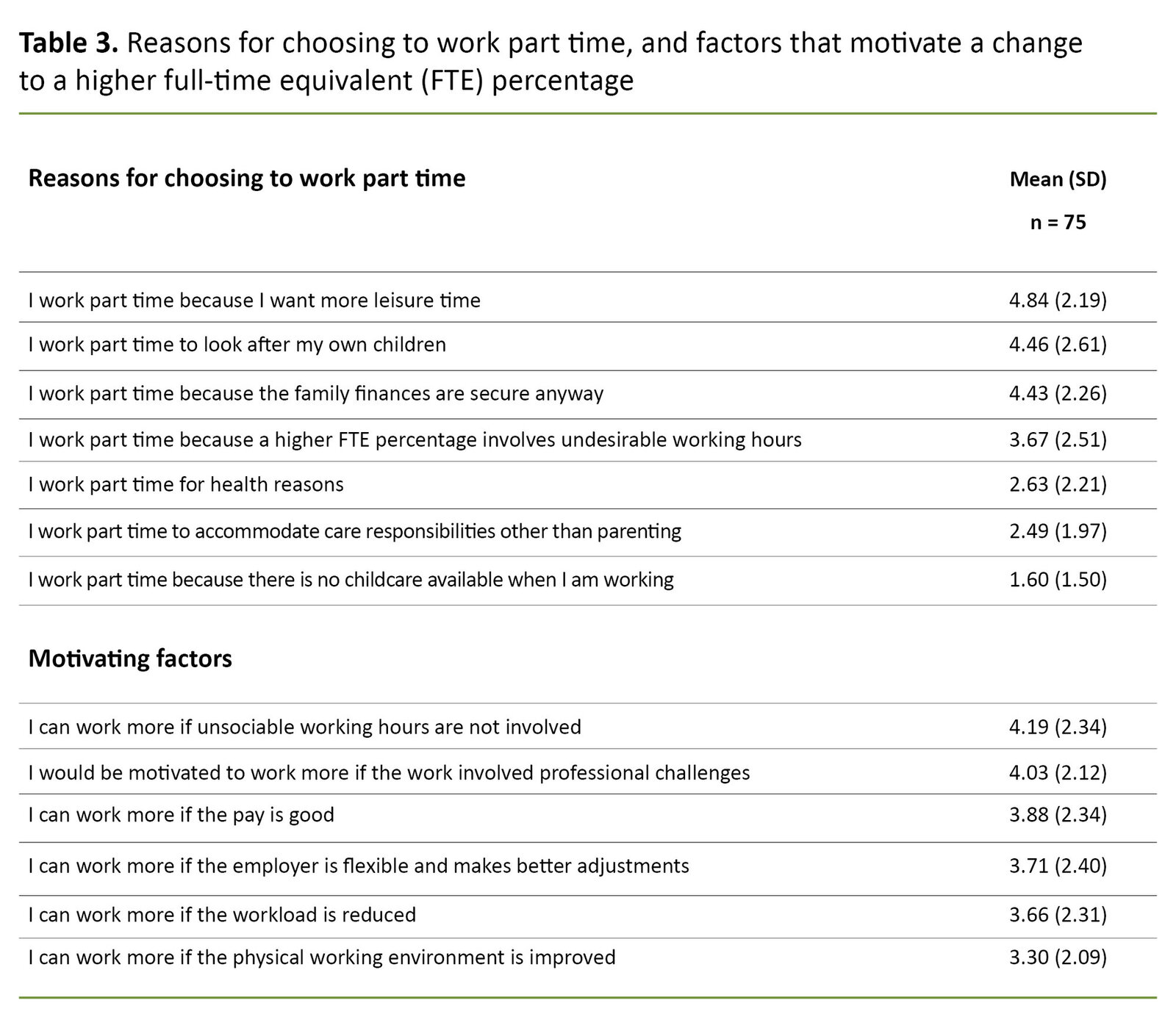
We asked part-time staff about their reasons for choosing to work part time, and what it would take for them to consider increasing their FTE percentage (table 3). Most of them had chosen to work part time in order to have more leisure time. Parenting responsibilities and secure finances were other important reasons.
Unsociable working hours was the most important barrier to the part-timers choosing a higher FTE percentage. Professional challenges were highlighted as a motivating factor for choosing a higher FTE percentage. Good pay and employer flexibility were also motivating factors, but to a somewhat lesser extent.
Binary logistic regression
We also investigated how the RNs’ priorities matched their choice of FTE percentage. FTE percentage was a dependent variable where 1 was coded as full time (= 100 per cent) and 0 as part time (<100 per cent). Independent variables were continuous factor scores estimated using Bartlett’s method.
We analysed associations by means of binary logistic regression, where the various factor scores were analysed concurrently. We found that factor 1 (job content) and factor 3 (contextual circumstances) related positively to full-time work, but the results were not statistically significant (odds ratio (OR) 1.2 [95% confidence interval (CI): 0.87–1.57], p = 0.276 and 1.2 [95% CI: 0.98–1.51], p = 0.115 respectively).
Factor 2 (family considerations) was inversely related to full-time work and was statistically significant (OR 0.6 [95% CI: 0.42–0.74], p = 0.000). The estimates changed little after we had controlled for age, partnership/marriage and parenting responsibilities for children under twelve years of age.
Discussion
The study’s objective was to shed light on the factors that influence the FTEs worked by RNs, and to gain an insight into what factors may motivate part-time employees to increase their FTE percentage. We have interpreted the total analysis and found that the main factors that influence the nurses’ choice of FTE percentage are job content, family considerations and contextual circumstances.
Both full-time and part-time nurses cite professional norms as a good reason for their choice of FTE percentage. Lifestyle and family values are the most important reasons for choosing part-time work, while sociable working hours is the factor that is most likely to encourage part-time staff to increase their FTE percentage.
Our part-time analysis indicates that while there is one group of nurses who may be influenced by adjustments made by the employer, there is another group who are less inclined to be influenced in the same way. Binary logistic regression showed that family considerations were inversely related to full-time work.
Factors that influence the choice of job
The respondents considered it important that their job was interesting and meaningful, and that it provided professional challenges. Family considerations meant that they appreciated the opportunity to choose between full-time and part-time work. Having the option to choose their own FTE percentage was a motivating factor for their choice of profession. Being able to adjust the FTE percentage to one’s life situation is considered to be important, and the opportunity to make such adjustments is utilised when family circumstances change.
The view that it is most appropriate for the woman to stay at home while the children are young, is a contextual circumstance. Another is the view that pay is important for the choice of FTE percentage, and that the rate of pay should determine which partner/spouse should work part time.
However, many RNs who have recently graduated are forced to accept part-time positions because they are unable to find full-time work. They are unable to choose their working time, but know that part-time work is a possibility. This situation may be seen to constitute not only involuntary part-time working, but forced part-time working.
It is interesting that the questions relating to pay load on the same factor as the statement ‘it is most appropriate for the woman to stay at home with the children while they are young.’ We assume that RNs reconsider their position from time to time and that they can therefore be influenced by, for example, changes to their rate of pay.
Reasons for choosing to work part time
Meaningful work that offers professional challenges is important to the respondents. This finding matches earlier research (13). We also find that lifestyle and family values are the most important reasons for working part time. A majority work part time because they want more leisure time and because the family finances are secure, which is also in line with earlier findings (7). However, our study does not distinguish between the financial situation of individuals and families.
Caring for children is also a reason for choosing to work part time (11, 12). The opportunity to adjust to one’s personal life situation is more important to part-timers than to full-timers when it comes to choosing their FTE percentage. Also, far more part-time staff have changed their working time as a consequence of changed family circumstances. The findings are significant and lead to two main conclusions: the most important reason for choosing to work part time is that they cherish their family and their leisure time.
It is also problematic that a higher FTE percentage often involves more unsociable working hours. Combining shift work with family life can be challenging. RNs work when others have time off, which makes it difficult to follow up on children’s leisure activities (14). Also, part-time staff are often assigned to a heavier shift pattern, and extra shifts introduce unpredictability (14).
Extra shifts are often more awkward because the employer is struggling to find cover for unsociable hours. In other words, the choices are directed by cultural and structural influences rather than being made by the nurses themselves (21).
Some can be encouraged to accept a higher full-time equivalent percentage
Nevertheless, some part-timers can be motivated to take on a higher FTE percentage provided their preferences are taken account of. We are unable to point to a single decisive factor that can make part-time nurses increase their FTEs. However, more sociable working hours, professional challenges, good pay and employer flexibility are all motivating factors.
The fact that pay, employer adjustments and flexibility influence the wish to increase FTEs, matches earlier findings (12). It is particularly interesting that professional challenges can motivate an increase of FTE percentage. At the same time, part-time staff are less involved with professional development opportunities, which may not be favourable for patients (12).
Workplaces with a large part-time workforce experience a weaker professional environment (2, 4). If institutions are set up to mainly accommodate full-time working, more employees will tend to ‘choose’ full-time jobs due to the opportunities for professional development. This would have a positive effect on professional standards, levels of pay and pension earnings, as well as gender equality (2, 6, 7, 29).
Some part-timers want to work part time
It is an interesting finding that part-time staff make up two distinct groups, one of which can be influenced by employer adjustments, while the other is less inclined to be thus affected. Those who are less influenced by employer adjustments point out that they are financially secure, and that they value their leisure time.
They also point out that an offer of a higher FTE percentage involves working shifts at undesirable times. Moreover, they would like to look after their children, which is challenging if they often have to work unsociable hours. However, full-time work is not necessarily more stressful than part-time work if individual circumstances are accommodated when rosters are drawn up (2, 14).
The factors that concern job content and contextual circumstances were positively related to full-time work. It is interesting that contextual circumstances were positively related to full-time work. Nurses make different priorities depending on their situation in life. They are weighing up the negatives and the positives, and more unsociable working hours will probably be considered a negative. However, the results were not statistically significant.
Family considerations were inversely related to full-time work, which means that the nurses were more likely not to choose to work full time. The nurses appreciated being able to adjust their own FTE percentage. They made use of this opportunity, which may be considered working part time voluntarily. For some, this opportunity was a motivating factor in their choice of profession. Employers should therefore continue to offer part-time work where this is desirable.
The challenges involved with building a full-time culture
However, we may ask whether this is a genuine choice. A change from part-time to full-time working must be seen in connection with cultural and structural frameworks (21). There is great demand among employers for the expertise offered by RNs, and the trade unions are fighting for full-time jobs. Building a full-time culture requires a range of actions and efforts to tackle the part-time culture, professional norms and attitudes (15).
Those who responded positively to employer adjustments are looking for a smaller workload, which is a challenge considering the shortage of RNs. Wider distribution of unsociable shifts will reduce the load on each individual (30).
The employer can facilitate full-time working
The employer is responsible for maintaining the quality of health services. However, the standard of services may be adversely affected if there is a predominance of part-time nurses. This suggests that full-time jobs should be the norm in order to maintain an overview and secure continuity vis-à-vis patients. The employer’s challenge is to accommodate the nurses’ various preferences.
The employer should prioritise the preferences which were found by the study to be positively related to full-time work: job content and contextual circumstances. The employer should especially focus on job content and ensure that nursing competencies are used to perform nursing tasks. This may influence recruitment as well as the quality of services.
Consideration must be given to how RNs will respond to institutional processes. Both full-timers and part-timers hold the opinion that contextual circumstances, such as pay, are important to their choice of FTE percentage. Similarly, professional challenges motivate acceptance of a higher FTE percentage and benefit the patients (2–5). The employer should consider these factors in order to contribute to the recruitment of new RNs and prevent existing RNs from leaving their profession.
Method discussion
The sample was skewed in that the majority of respondents were working full time. One of the study’s weaknesses is its low response rate. No reminders were issued, and the representativeness of the sample has not been considered. The study was conducted within the bounds of the municipal health service and includes no hospital employees. The findings only apply to the priorities of RNs who work in municipal and private institutions, and to factors that influence their FTE percentage.
Further research should include hospital employees, and barriers to full-time working should be surveyed among various groups of nurses. It is a weakness that FTE percentages were not specified for part-time positions. Additionally, it was not specified whether part-time working was a voluntary choice or an undesirable adjustment. Neither was it made clear what share of the sample work shifts or daytime only.
We devised the questionnaire ourselves due to insufficient familiarity with validated and reliability-tested forms within the field. The form is based on new institutional theory and our knowledge of the field (21). The loadings and Cronbach’s alpha for the total analysis were low. Caution should therefore be taken when drawing conclusions from this analysis, particularly with reference to factors 2 and 3.
Conclusion
Job content, family considerations and contextual circumstances influence the full-time equivalent percentage worked by registered nurses. Sociable working hours and professional challenges are factors that may motivate part-time employees to increase their full-time equivalent percentage.
I am grateful to the informants for their important contributions to this study. I am also grateful to statistician and associate professor Roy Miodini Nilsen for his assistance with the statistical analyses and to professor Oddbjørn Bukve for his input to the manuscript. Both work for the Western Norway University of Applied Sciences.
References
1. Dolonen KA. 5900 sykepleiere og spesialsykepleiere mangler i helsevesenet. Sykepleien; 05.05.2018. Available at: https://sykepleien.no/2018/05/5900-sykepleiere-og-spesialsykepleiere-mangler-i-helsevesenet (downloaded 12.03.2019).
2. Ingstad K. Hele og delte sykepleiere: En kvalitativ studie av sykepleieres arbeidsvilkår og arbeidstid i sykehjem. (Doktoravhandling.) Trondheim: Norges teknisk-naturvitenskapelige universitet, Fakultet for samfunnsvitenskap og teknologiledelse, Institutt for sosialt arbeid og helsevitenskap; 2011. Available at: https://brage.bibsys.no/xmlui/handle/11250/267842 (downloaded 22.03.2019).
3. Hallandvik JE, Olsen T. Heltid – løsning eller problem? Sluttrapport fra evalueringen av heltidsprosjektet i Kristiansand kommune. Kristiansand: Universitetet i Agder; 2011. Rapport 157/2011. Available at: http://hdl.handle.net/11250/135085 (downloaded 22.03.2019).
4. Moland LE, Bråthen K. Hvordan kan kommunene tilby flere heltidsstillinger? Oslo: Forskningsstiftelsen Fafo; 2012. Report 14/2012. Available at: https://www.fafo.no/index.php/zoo-publikasjoner/fafo-rapporter/item/hvordan-kan-kommunene-tilby-flere-heltidsstillinger (downloaded 22.03.2019).
5. Moland LE. Heltid-deltid – en kunnskapsstatus. Oslo: Forskningsstiftelsen Fafo; 2013. Rapport 27/2013. Available at: https://www.fafo.no/index.php/zoo-publikasjoner/fafo-rapporter/item/heltid-deltid-en-kunnskapsstatus (downloaded 22.03.2019).
6. Ingstad K, Kvande E. Må sykepleieryrket være et deltidsyrke? Nordisk sygeplejeforskning. 2011;1(03):206–18.
7. Nicolaisen H. Løsninger på deltidsutfordringen – ingen «quickfix». Søkelys på arbeidslivet. 2013;30(1–2):151–7.
8. Meld. St. 29 (2010–2011). Felles ansvar for eit godt og anstendig arbeidsliv. Oslo: Arbeids- og sosialdepartementet; 2011. Available at: https://www.regjeringen.no/no/dokumenter/meld-st-29-20102011/id653071/ (downloaded 22.03.2019).
9. Norsk Sykepleierforbund. Kompensasjon for ubekvem arbeidstid og forskjøvet arbeidstid. Oslo; 2018. Available at: https://www.nsf.no/vis-artikkel/113721/17074/Kompensasjon-for-ubekvem-arbeidstid-og-forskjovet-arbeidstid (downloaded 22.03.2019).
10. Egeland C, Drange I. Frivillig deltid – kun et spørsmål om tid? Oslo: Arbeidsforskningsinstituttet; 2014. Report 4/2014. Available at: https://doi.org/10.7577/afi/rapport/2014:4 (downloaded 22.03.2019).
11. Køber T, Vigran Å. Arbeidstid blant helsepersonell, stort omfang av deltidsarbeid. Samfunnsspeilet. 2011;25(2):58–62. Available at: https://www.ssb.no/arbeid-og-lonn/artikler-og-publikasjoner/stort-omfang-av-deltidsarbeid (downloaded 12.03.2019).
12. Moland LE. Ønsket og uønsket deltid – konsekvenser for arbeidstaker, arbeidsgiver og tjenestetilbud. Oslo: Forskningsstiftelsen Fafo; 2009. Report 15/2009. Available at: https://www.fafo.no/index.php/zoo-publikasjoner/fafo-rapporter/item/onsket-og-uonsket-deltid-konsekvenser-for-arbeidstaker-arbeidsgiver-og-tjenestetilbud (downloaded 22.03.2019).
13. Christiansen B, Bjørk IT. Godt – eller godt nok? Hvordan opplever sykepleiere idealer og realiteter i utøvelsen av yrket? Nordisk tidsskrift for helseforskning. 2016;12(1):64.
14. Abrahamsen B, Holte KA, Laine M. Work-family interference: nurses in Norway and Finland. Professions and Professionalism. 2012;2(1):60–74.
15. Ingstad K. Turnus som fremmer heltidskultur. Oslo: Gyldendal Akademisk; 2016.
16. Ingstad K, Kvande E. Arbeid i sykehjem – for belastende for heltid? Søkelys på arbeidslivet. 2011;28(1–2):42–55.
17. Ingstad K, Amble N. En ny ro med langturnus. Less job stress with 12-hour shifts. Nordic Journal of Nursing Research. 2015;35(3):152–7.
18. Harris R, Sims S, Parr J, Davies N. Impact of 12 h shift patterns in nursing: A scoping review. International Journal of Nursing Studies. 2015;52(2):605–34.
19. Bae S-H, Fabry D. Assessing the relationships between nurse work hours/overtime and nurse and patient outcomes: systematic literature review. Nursing Outlook. 2014;62(2):138–56.
20. Dall’Ora C, Ball J, Recio-Saucedo A, Griffiths P. Characteristics of shift work and their impact on employee performance and wellbeing: a literature review. International Journal of Nursing Studies. 2016;57:12–27.
21. Scott WR. Institutions and organizations: ideas, interests, and identities. 4. ed. Thousand Oaks, California: Sage Publications; 2014.
22. Polit D, Beck C. Nursing Research: generating and assessing evidence for nursing practice. 10. ed. Philadelphia: Wolters Kluwer; 2017.
23. Ringdal K. Enhet og mangfold. Samfunnsvitenskapelig forskning og kvantitativ metode. 3. ed. Bergen: Fagbokforlaget; 2013.
24. Bjørndal A, Hofoss D. Statistikk for helse- og sosialfagene. Oslo: Gyldendal Akademisk; 2004.
25. Pett MA, Lackey NR, Sullivan JJ. Making sense of factor analysis: the use of factor analysis for instrument development in health care research. Thousand Oaks, California: Sage Publications; 2003.
26. Pallant J. SPSS survival manual: a step by step guide to data analysis using SPSS. 4. ed. Maidenhead: McGraw-Hill International; 2010.
27. De nasjonale forskningsetiske komiteene. Forskningsetiske retningslinjer for samfunnsvitenskap, humaniora, juss og teologi. Oslo; 2016. Available at: https://www.etikkom.no/forskningsetiske-retningslinjer/Samfunnsvitenskap-jus-og-humaniora/ (downloaded 22.03.2019).
28. World Medical Association. Helsinkideklarasjonen. Fortaleza, Brazil; 2013. Available at: https://www.etikkom.no/forskningsetiske-retningslinjer/Medisin-og-helse/Helsinki-deklarasjonen/ (downloaded 12.03.2019).
29. Moland LE. Større stillinger og bedre drift. Evaluering av programmet ufrivillig deltid. Oslo: Forskningsstiftelsen Fafo; 2015. Report 25/2015. Available at: https://www.fafo.no/index.php/zoo-publikasjoner/fafo-rapporter/item/storre-stillinger-og-bedre-drift (downloaded 22.03.2019).
30. Amble N, Ingstad K. Helgearbeid og heltidskultur. Sykepleien; 16.01.2015. Available at: https://sykepleien.no/meninger/innspill/2015/01/helgearbeid-og-heltidskultur (downloaded 12.03.2019).










Comments